A patient comes in with a bombed-out molar, writhing in pain. They look at you with pleading eyes and ask, “Doc, can you just save it?”
Our instinct, our training, everything in us wants to be the hero. But what if I told you that sometimes, the best endo is no endo at all?
If you’ve ever heroically “saved” a tooth only to have it fail catastrophically a year later, this is for you. We’re not just talking about the how of endodontics; we’re talking about the when and, more importantly, the when not to.
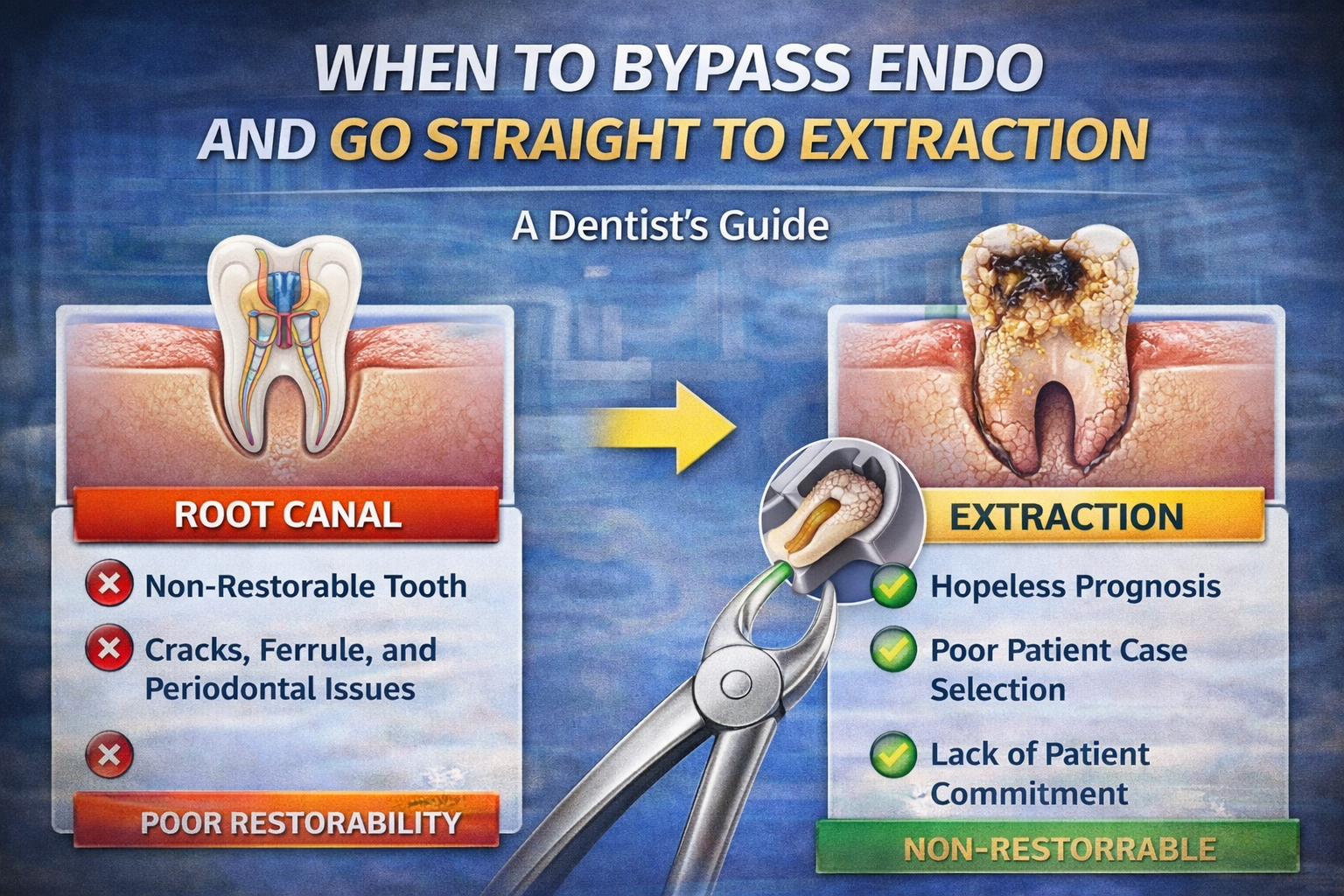
This is a clear, objective checklist to help you confidently identify when bypassing endo and going straight to an extraction is the better, more predictable, and more ethical service for your patient and your practice.
The Foundational Principle: Can the Tooth Be Predictably Restored?
A perfect root canal on a non-restorable tooth is a complete and total failure. Endodontic treatment only makes sense if the tooth can be returned to function for the long term. Before you ever pick up a file, you must be a ruthless diagnostician of restorability.
Here are the absolute clinical red flags.
1. Subcrestal Caries or Fractures
If decay or a crack extends below the level of the bone, you are in a nearly impossible situation. You cannot bond to a bleeding, contaminated surface, and you cannot create a clean margin. Violating the biologic width leads to chronic inflammation, bone loss, and eventual failure.
- Pro Tip: Use a CBCT or high-quality transillumination to identify hidden cracks before you commit to treatment.
2. Inadequate Ferrule
The textbook rule is clear: you need 1.5 to 2mm of solid, circumferential tooth structure above the margin to create a ferrule that resists fracture. If, after removing all decay and considering crown lengthening, you cannot achieve this, the prognosis plummets. A post and core in a tooth with no ferrule will eventually act like a wedge and split the root.
3. Compromised Crown-to-Root Ratio
After accounting for any necessary crown lengthening, will the final crown be longer than the root embedded in bone? A crown-to-root ratio of less than 1:1 puts the tooth under extreme biomechanical stress and dramatically increases the risk of failure.
4. Hopeless Structural or Periodontal Issues
- Cracks: A crack that can be traced across the pulpal floor or into the furcation is a ticking time bomb.
- Perforations: Large iatrogenic perforations from previous endo attempts, especially those below the crestal bone, carry a very poor prognosis.
- Periodontal Status: A combined perio-endo lesion with circumferential pocketing (>6mm), Grade II/III mobility, or vertical bone loss involving the furcation often has a hopeless prognosis. You cannot build a solid house on a crumbling foundation.
Patient-Related Factors: When a “Good” Tooth is a Bad Case
Even a clinically perfect case can be a terrible choice if the patient isn’t the right candidate.
1. Poor Oral Hygiene or Uncontrolled Systemic Disease
A patient with consistently poor hygiene, uncontrolled diabetes, or unmanaged bruxism has a biological environment that is set up for failure. The risk of recurrent decay or fracture around that heroically saved tooth is incredibly high.
2. The “Crown Later” Patient (A Non-Negotiable Rule)
This is one of the most important rules you must have: Never perform a root canal unless the patient has also financially committed to the final crown.
A root-canaled tooth without a crown is a temporarily saved tooth that is destined to fracture. If a patient says they’ll “get the crown later,” you are being set up for a future failure that will be blamed on you. The root canal and the crown are two parts of a single procedure. If they won’t commit to the complete treatment, the root canal itself is not a viable option.
The Communication: How to Explain Your Decision with Confidence
When you’ve determined that an extraction is the most predictable option, you need to communicate this to a patient who may be emotionally invested in “saving” their tooth. Be empathetic, confident, and direct.
Here is a simple script:
“Mrs. Jones, I know your goal is to save this tooth, and I want to do what’s best for you in the long run. We can technically do a root canal here, but the foundation of the tooth is very weak due to this deep crack. Based on my experience, I can’t promise you this treatment will last. I’m concerned you would be investing a significant amount of time and money into something that might fail in just a year or two.”
“I believe the better, more predictable long-term option would be to remove this compromised tooth and replace it with a dental implant, which has a much higher and more predictable long-term success rate.”
Your job is not just to be a technician who can save any tooth; it’s to be a wise diagnostician who knows which teeth are worth saving.